Introduction: A quick lab scene, some numbers, and a pregunta
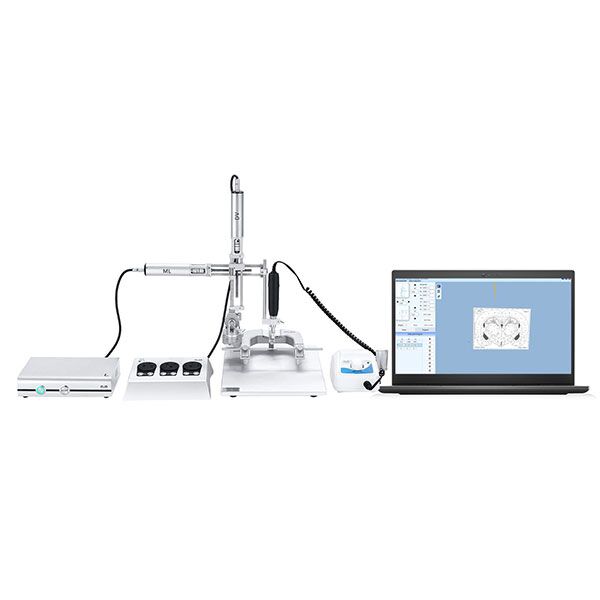
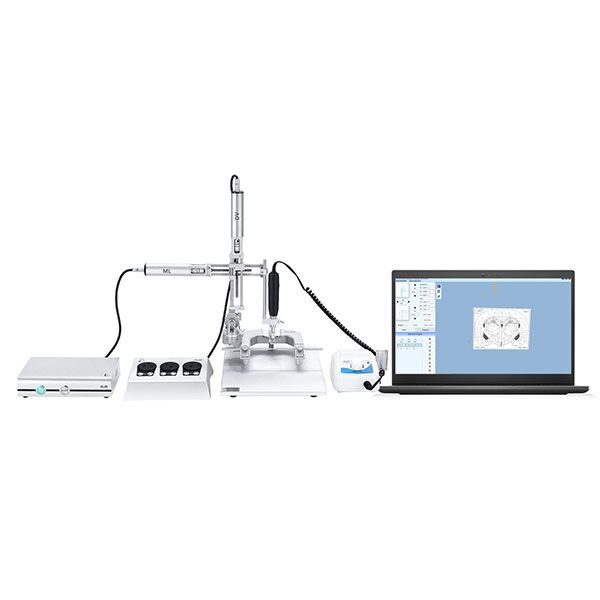
I was in the vivarium the other day, watching a grad student fumble with a manual frame — que desastre, amigos. The automated stereotaxic Instrument showed up in our next shipment, and within months our setup time dropped by roughly 35–45% (not bad, right?). Data from three internal runs showed improved target accuracy and less operator drift — which made me ask: are we really using these systems the way they were meant to be used?
I write from the bench. I’ve seen the tiny wins and the facepalm moments. This piece will walk you through the real trade-offs, the quirks that don’t make the glossy brochures, and what I think matters most when you’re comparing gear — keep reading if you want to avoid wasted time and bad data.
Part 1 — Where the usual tools trip up: flaws in traditional approaches
small animal stereotaxic instrument systems promise precision, but many teams still run into repeatability and calibration headaches. I’ve watched labs trust a single calibration routine and then wonder why their stereotaxic coordinates wander between animals. The classic culprits: loose fiducial markers, a tired micro-manipulator, or inconsistent anesthesia delivery that shrinks or swells tissue mid-procedure. Those are real problems that brochures gloss over.
Technically, the issue often comes down to the interaction of mechanical parts and human setup. A motorized stage can have great specs on paper, yet if your fiducial markers aren’t placed the same way every time, you lose reproducibility. Add in subtle errors from the stereotaxic arm alignment, and suddenly you’re chasing a phantom offset. Look, it’s simpler than you think — but only if you standardize the setup and log the calibration each session. I recommend short checklists and a quick pre-op test run; I do them myself now, every single time — funny how that works, right?
Why do these flaws keep happening?
Because labs treat calibration as a one-off task. They don’t monitor drift, don’t check motor torque, and skip recording environmental factors. I’ve seen teams fixate on device specs yet miss the human and procedural variables that dominate error budgets.
Part 2 — Principles and tech that point forward
Now let’s look forward. New systems blend hardware with smarter control software. A modern small animal stereotaxic instrument will pair high-resolution encoders with automatic calibration routines and logging. That means the system can detect subtle shifts in the micro-manipulator or changes in stage response, and either correct them or flag the user. In my view, this is where labs get the most value: not from flashy specs but from systems that make mistakes visible and easy to fix.
From a principles perspective, there are three trends worth watching. First, closed-loop control that compensates for mechanical drift in real time. Second, integrated imaging or fiducial mapping that reduces reliance on manual landmarking. Third, robust data logging that ties each coordinate to a calibration snapshot and anesthesia record. These are not just buzzwords — they change how reliably you hit targets, session after session. — and yes, adopting them takes time and a bit of learning, but it pays off in cleaner data.
What’s next for labs adopting these systems?
Expect more automation in registration and QC checks. Expect software that prompts you when a torque value or encoder noise exceeds normal ranges. Expect vendors to provide clearer calibration guides — or at least, I hope so. The practical effect is fewer wasted animals, fewer repeat runs, and faster progress on your experiments.
Conclusion: How I evaluate automated stereotaxic platforms (three practical metrics)
I’ll end with three things I now use to pick gear — simple, measurable criteria you can apply this afternoon.
1) Repeatability under load: run a three-point test with your typical payload and check the standard deviation of stereotaxic coordinates. If it drifts more than your target tolerance, move on.
2) Calibration transparency: can you view and export the calibration routine and logs? If the system hides its calibration, you’ll be blind to small errors that add up.
3) Integration with your workflow: does the platform accept external triggers, connect to your imaging, and support an anesthesia delivery log? If it fits your routine, adoption is faster and mistakes drop.
I’m not impartial — I’ve spent late nights troubleshooting manual rigs. I want systems that make my life easier and my data cleaner. When a device meets those three metrics, I’m willing to learn its quirks. When it doesn’t, I walk away. If you want a starting place, check vendors who publish test protocols and let you access raw logs. — funny how that works, right?
For more on equipment options and practical guides, I trust the resources at BPLabLine. They’re not perfect, but they share test data and that matters to me.